Epidermolysis bullosa

3. Odontology
In this section, we will discuss the significant effects of EB on the integrity and formation of teeth, dental supporting structures, and the oral mucosa.
The extent of oral involvement can vary depending on the subtype of EB. Some of the most important oral issues associated with EB include:
- Oral Mucosa Injuries: The mucosa lining the inside of the mouth is highly susceptible to blister formation due to constant rubbing and friction from food, liquids, objects, and even parts of the body. These blisters are quite painful and difficult to heal. Repairing these injuries is complicated because the mouth is constantly in use for speaking, eating, salivating, and even breathing, making it challenging to protect intraoral wounds to promote healing. As a result, they can progress to erosions and chronic ulcerations. For symptomatic treatment, preparations containing hyaluronic acid are commonly used to protect the injured areas, and anaesthetic preparations (such as lidocaine) may be applied in cases of severe pain.
- Ankyloglossia: This condition, characterized by difficulty extending the tongue, occurs when the lingual mucosa is attached to the bottom of the mouth. Ankyloglossia restricts tongue movement (both outward and toward the molars), interfering with swallowing and the articulation of words.
Microstomia: This refers to a small oral cavity and limited mouth opening. As blisters and erosions in the oral mucosaheal, they can retract, reducing the ability to open the mouth. Initially, microstomia may go unnoticed, but it can lead to significant repercussions for nutrition and medical treatments (such as difficulties managing the airway during anaesthesia and challenges for dentists in accessing the mouth to treat dental issues).
- Gingival Blisters and Erosions: The gums are also prone to blistering, particularly in certain subtypes of EB, leading to problems with tooth structure and distribution.
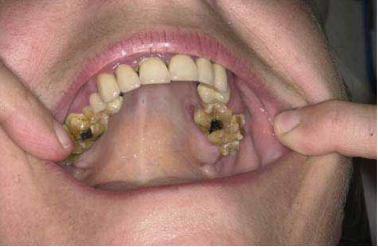
- Dental Enamel Hypoplasia and Dysplastic Teeth: The mutations in the proteins responsible for the structural issues of the skin and mucous membranes in EB also contribute to inadequate odontogenesis (the growth and maturation process of teeth). Enamel hypoplasia, which is the insufficient development of the outermost layer of the tooth, is seen in some types of EB, while others may present with normal enamel structure.
- Recurrent Cavities: The recurrence of cavities is a common issue in the more severe forms of EB. This problem is multifactorial, arising from poor oral hygiene due to intraoral wounds (exacerbated by microstomia and pain), the presence of contractures from scarring, limited tongue mobility, a diet of soft foods (which tend to stick more to the teeth), and difficulties in swallowing.
- Premature Tooth Loss: Children with EB often experience earlier tooth loss due to structural and developmental issues associated with the disease.
Premature tooth loss: Children with EB usually lose their teeth earlier due to structural and developmental problems associated with the disease.
To prevent or delay these complications, proper oral care is essential, starting with early referral to a dentist between 3 to 6 months of age. Education on daily tooth brushing should be provided, using a small-headed toothbrush with soft bristles. The use of fluoride is recommended to help prevent cavities, and chlorhexidine may be used in cases of gingivitis. Regular dental check-ups are crucial for ongoing management.