Epidermolysis bullosa

10. Cancer
Cancer begins when cells in the body begin to grow out of control. Most skin cancers start in the epidermis, which is the top layer of the skin. There are three main types of skin cancer:
- Squamous cell carcinoma (SCC): it originates in the keratinocytes, which are the cells of the epidermis that are constantly shed as new cells are formed.
- Basal cell carcinoma: it originates from the basal cells, which are the cells that are in the lower part of the epidermis.
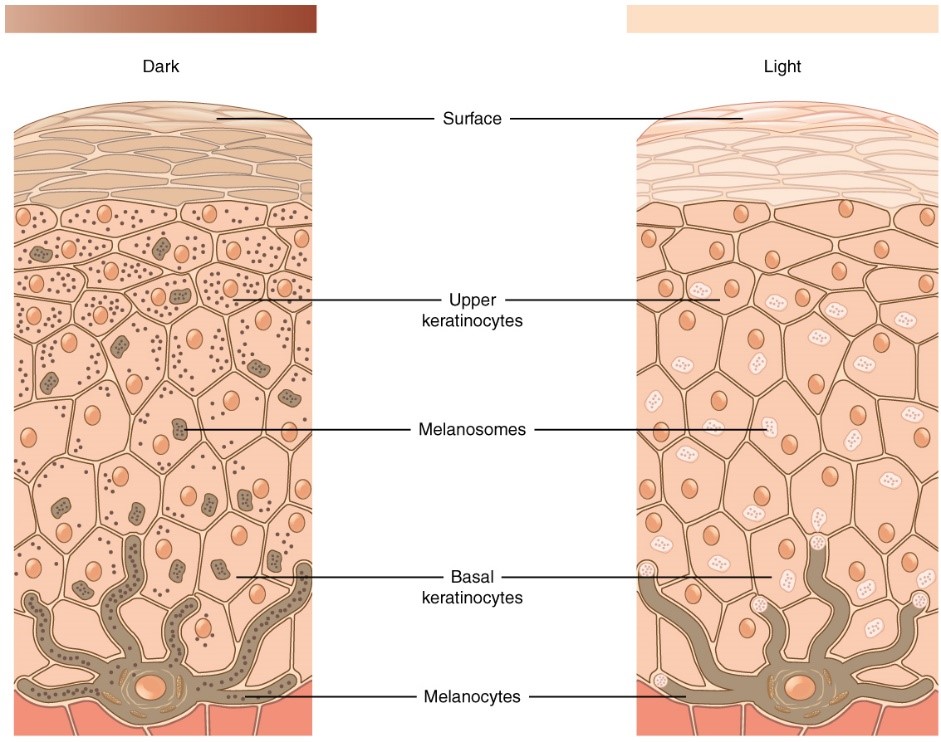
Malignant melanoma: it originates from melanocytes, which are the cells that produce the brown pigment called melanin. Melanin acts as a natural sunscreen and protects the deeper layers of the skin against some of the harmful effects of the sun.
Patients with severe dystrophic EB have a higher risk of developing a skin SCC. Today we know that SCC is a frequent complication in EB, specifically of the severe dystrophic EBs. The characteristics of SCC which appear in these patients are:
- Early age appearance: the risk gets higher with age. Risk of 7.5% at 20 years old, 67.8% at 35 years old and 90% at 55 years old.
- The injuries appear in areas of chronic ulcers and scars.
- The injuries are located in the extremities, especially in hands and feet.
- Multiple injuries, with an average of 3-3.5 tumour.
- Difficult diagnostic: the SCC can present itself as a chronic ulcer, a more painful than usual ulcer, a bump, a scab area (hyperkeratosis) or it might look like a wart. It is compulsory to perform a skin biopsy in any suspicious injury and sometimes it should be done on several close to the injury areas, as sometimes it is not easy to detect the squamous cells carcinoma.
- Poor prognosis: local recurrences and development of metastases. Today this complication is the leading cause of death in patients with severe dystrophic EB.
SCC is less frequent, of later appearance and less aggressive in the other types of recessive dystrophic EB, dominant dystrophic EB, intermedia junctural EB and in Kindler’s EB. Patients with simple EB do not have a higher risk of SCC.
Although the patients with severe dystrophic EB have a higher risk of SCC in oral mucosa, these are rare. It is advised to have periodic controls with a full revision of the skin to detect early any suspicious injuries. The SCC development mechanism in patients with EB is unknown, even with all the investigations done up to the moment.
Treatment of SCC
- Surgery: complete extirpation is the treatment of choice. Another surgical technique is the minimally invasive surgery (Mohs’s surgery). Due to the frequency of the injury in the extremities, many times it is necessary to amputate the extremity.
- Radiotherapy
- Conventional chemotherapy
- Biological treatments: cetuximab and rigosertib.
While we do not know the reason for its aggressiveness with local recurrence and its metastases capacity, many times the current treatments are palliative.
All the cases of patients with EB and SCC must be evaluated by multidisciplinary units in which, at least, there must participate specialists in dermatology, surgery, pathological anatomy, oncology, rehabilitation and psychology.