Gliomatosis cerebri

Diagnosis
GC should be suspected when a child presents with symptoms. Brain imaging should be ordered when it is suspected, and should be interpreted in the clinical context and other diagnostic tests.
A surgical biopsy performed by an experienced team in a referral centre is the only way to confirm –or rule out- the diagnosis of GC. The tissue material obtained and the way it is stored is very important not only for diagnostic purposes, but also for research projects. Biopsy from a single site can be non-representative from the whole tumour, which is why it is advisable to obtain at least two different biopsies using the same needle tract at different depths of the tumour. This procedure involves surgery, and every surgery involves risk. You should have a detailed discussion with your medical team regarding the risks and benefits of performing a surgical biopsy.
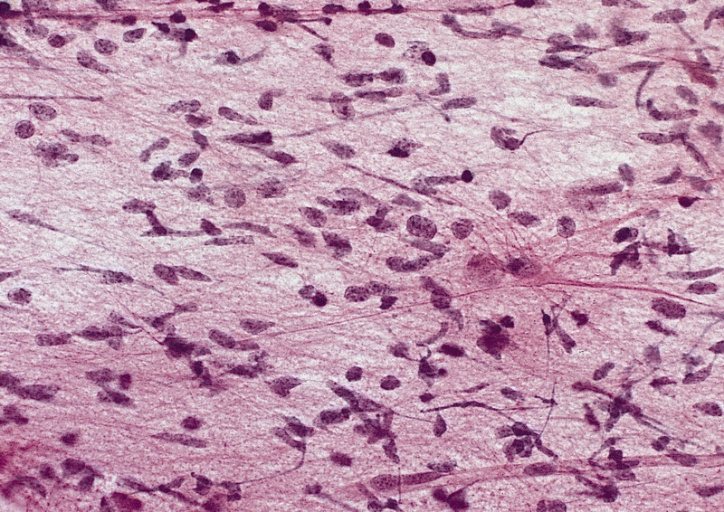
A histologic review of the samples describes a glial tumour with a determined “grade”. Glial tumours are usually graded based upon a number of criteria observed with optic microscopy. Low grade gliomas (LGG) include grades I and II. High grade gliomas (HGG) include grades III and IV. However, brain tumours are heterogeneous and a biologically aggressive glioma, irrespective of the histologic appearance, will have a poor prognosis for the patient in concordance with the biology of the tumour, not the morphologic characteristics under the microscope. In most GC cases, histologic review is compatible with a grade III or IV. However, some cases have been reported as grade II.
GC can be determined as astrocytoma, oligodendroma or a “mixed tumour” which is made up of both glia cell types (astrocytes or oligodendrocytes).
