Síndrome de Kabuki

2.1. Primary Skeletal Abnormalities
2.1.1. Joint Hypermobility
Joint Hypermobility or Hyperlaxity is observed in 50%-75% of individuals with Kabuki syndrome. Joint dislocations, especially in the hips, kneecaps, and shoulders, are not uncommon as a result. As with most conditions involving joint hypermobility, it is more prevalent in girls than in boys, and this finding improves with age.
A 32% prevalence has been described in patients with KMT2D mutations compared to 9% without mutations in this gene.
Marked hypermobility can lead to recurrent sprains, particularly in joints such as the ankle or wrist, although this is not common in Kabuki patients.
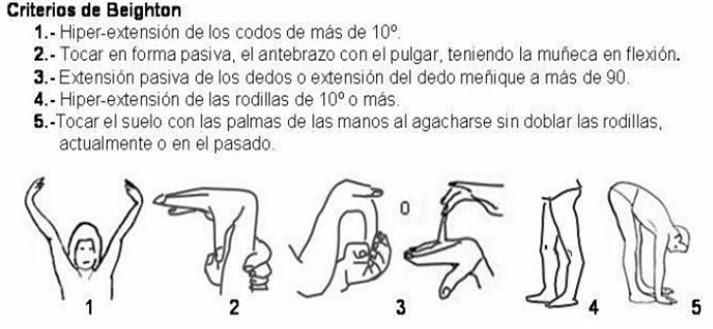
To assess whether a patient has joint hypermobility, the Beighton criteria are generally used. These consist of 5 maneuvers, all of which can be evaluated bilaterally except for touching the palms to the floor. A score greater than 4 points indicates that the person may have joint hypermobility.
Regarding its management, there is no specific and definitive treatment. The approach is based on informing, preventing (physical therapy is important), analgesia, and psychological support:
Establish a correct diagnosis and inform the patient
- Explain that it is a benign and non-disabling disorder, although it can be limiting in some cases
- Avoid over-diagnosis or psychogenic diagnosis
- Reduce anxiety and frustration
- Possible predisposition to chronic joint pain
Prevention:
- Avoid overloading the joints (obesity, carrying weights, etc.)
- Joint protection for sports
- Physical therapy exercises for strengthening and stretching muscles. Recommended: swimming, yoga
- Consult your primary care physician if symptoms worsen or increase
Treat what can be treated:
- Preference for local therapeutic measures: splints (wrist braces, elbow braces, ankle braces), injections (with caution), physical therapy, electrotherapy, and decontracting massage
- Physical measures: heat (muscle contracture) or cold (acute and recent injuries)
- Topical creams or gels
- Analgesics and non-steroidal anti-inflammatory drugs for a short period
- Treatment of anxious and/or depressive components (psychological therapy)
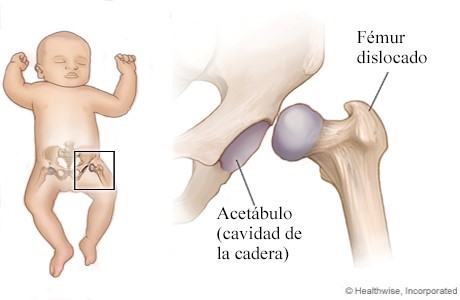
2.1.2. Congenital Hip Dysplasia
This can account for 6% of cases and is a condition where the hip joint is abnormal. Some babies with Kabuki syndrome are born with this malformation. In this condition, the head of the femur does not fit properly into the joint, which can lead to limping and pain later on. In more severe cases, this condition can be disabling.
The treatment will depend on the child's age and the severity. Mild cases improve without any treatment after several weeks. More severe cases will require treatment.
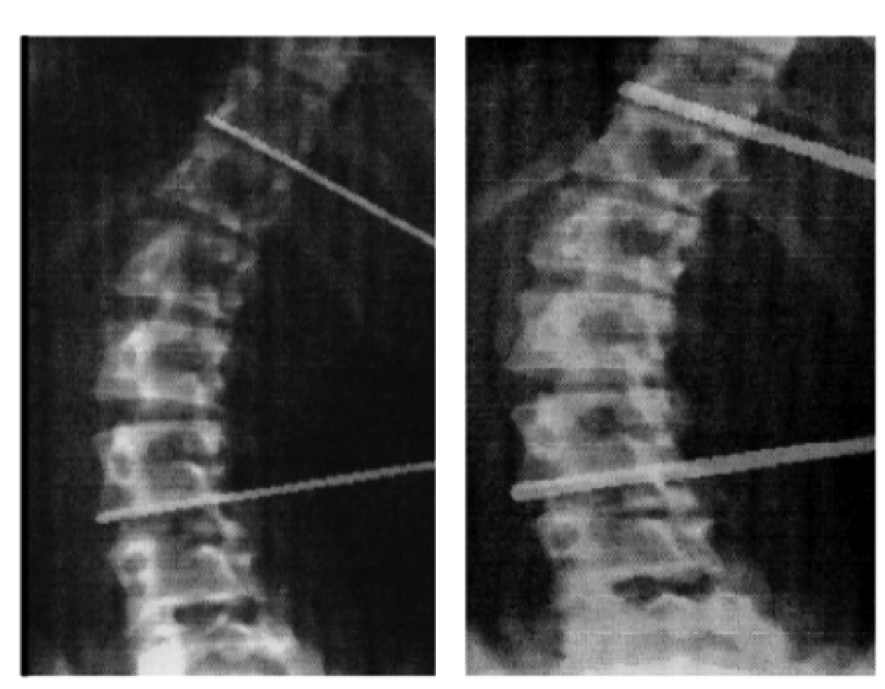
2.1.3. Vertebral Anomalies
These can account for 20% of cases and can cause scoliosis. Among them, hemivertebrae and "butterfly" vertebrae are notable.
Hemivertebra is the most common cause of congenital spinal anomalies and is defined as a disorder characterized by the congenital failure of a vertebra to fully develop, possibly caused by the complete failure of the chondral nucleus of a vertebral body.
2.1.4. Skeletal Abnormalities of Hands and Fingers
These can account for 87% of cases and include:
- Brachydactyly or short fingers (middle phalanges or metacarpals)
- Clinodactyly of the 5th finger
- Persistent fetal pads on the fingers
- Dermatoglyphic anomalies or grooves on the palms and soles
These characteristics rarely lead to clinical problems and are more often used as a clue for diagnosis.