Osteogenesis imperfecta

4. Bone fragility and fractures
Bone fragility
Bone fragility is the main problem for those affected by OI. Bone resistance to a fracture depends on bone composition (collagen characteristics, degree of mineralisation) and structure (size and shape, bone mass, quantity of cortical and trabecular bone).
In OI we see alterations at all levels: anomalous or deficient collagen, a low degree of mineralisation, thin and curved bones, low bone mass with attenuated cortex and little spongy trabeculae (Figure 11).

Types of fractures
A fracture is the loss of normal continuity in a bone or a cartilage. There are many types of fractures; in some in of them the bone is largely destroyed and others are essentially microscopic. In terms of the localisation of the fracture in the bone, we talk about diaphyseal, epiphyseal and metaphyseal fractures. Fractures may also be closed, when the bone is broken but not the surrounding skin, or open, when both the bone and the adjacent skin are broken. Open fractures are usually produced by high impact mechanisms, which is not typically the case in OI, and they have the added complication that, as the skin cannot provide protection, there is the possibility of infection.
If we have a look at the plane of fracture we can find:
- Transverse fractures: the fracture is perpendicular to the main axis of the bone.
- Spiral or hairline fractures: the fracture line is in the form of a spiral on the surface of the bone. Fractures of this kind are generally produced by torsion.
- Butterfly or oblique fracture: Generally produced by a traction-compression force on the bone. There are two oblique lines that leave a free triangular fragment.
- Comminuted fractures: the bone is broken into multiple small fragments.

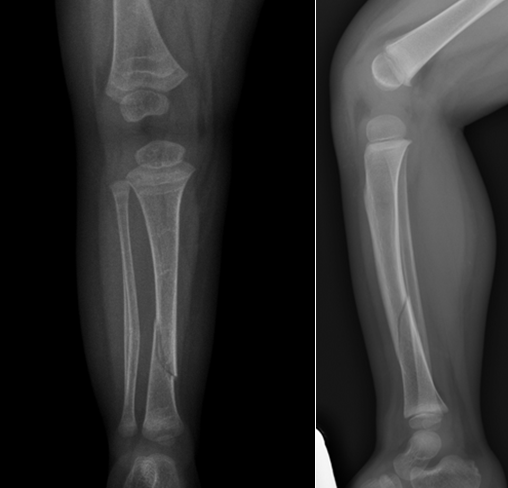
Fractures may also be classified as displaced when there is a separation or displacement of fragmented extremes, or non-displaced/aligned when the fragments remain in line with the main axis of the bone (Figure 16).

In children, we may distinguish some characteristic fractures:
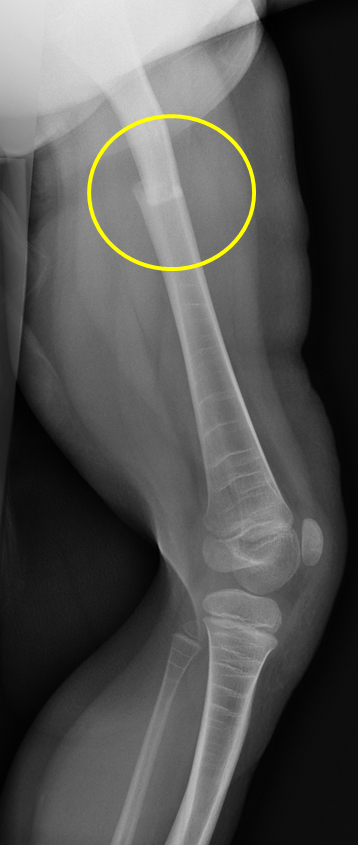
- Greenstick fracture: the bones are more elastic and they bend and crack, instead of breaking completely.

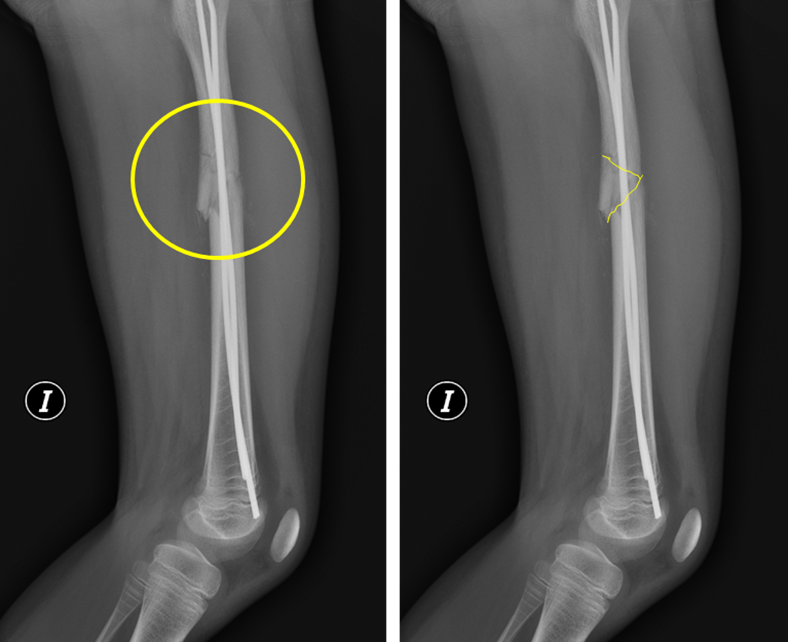
- Buckle fracture: the trabeculae break and the diametre of the bone is widened, folding on itself without breaking the cortex.

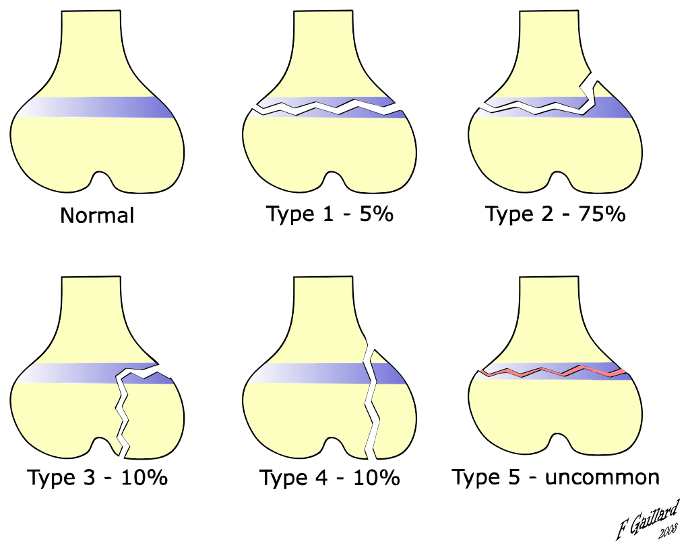
- Salter-Harris fracture: the physis is a weak point in the bone. In children, fractures in the epiphysal plate (through the growth cartilage) are common. Depending on the "line they draw on the bone", they are classified into 5 types (Figure 19):
Fractures in OI are usually transverse diaphyseal fractures in long bones or fractures at the maximum curvature point in deformed bones. Vertebral compression fractures are also frequent in OI.