Osteogenesis imperfecta

2.1. Lower limbs
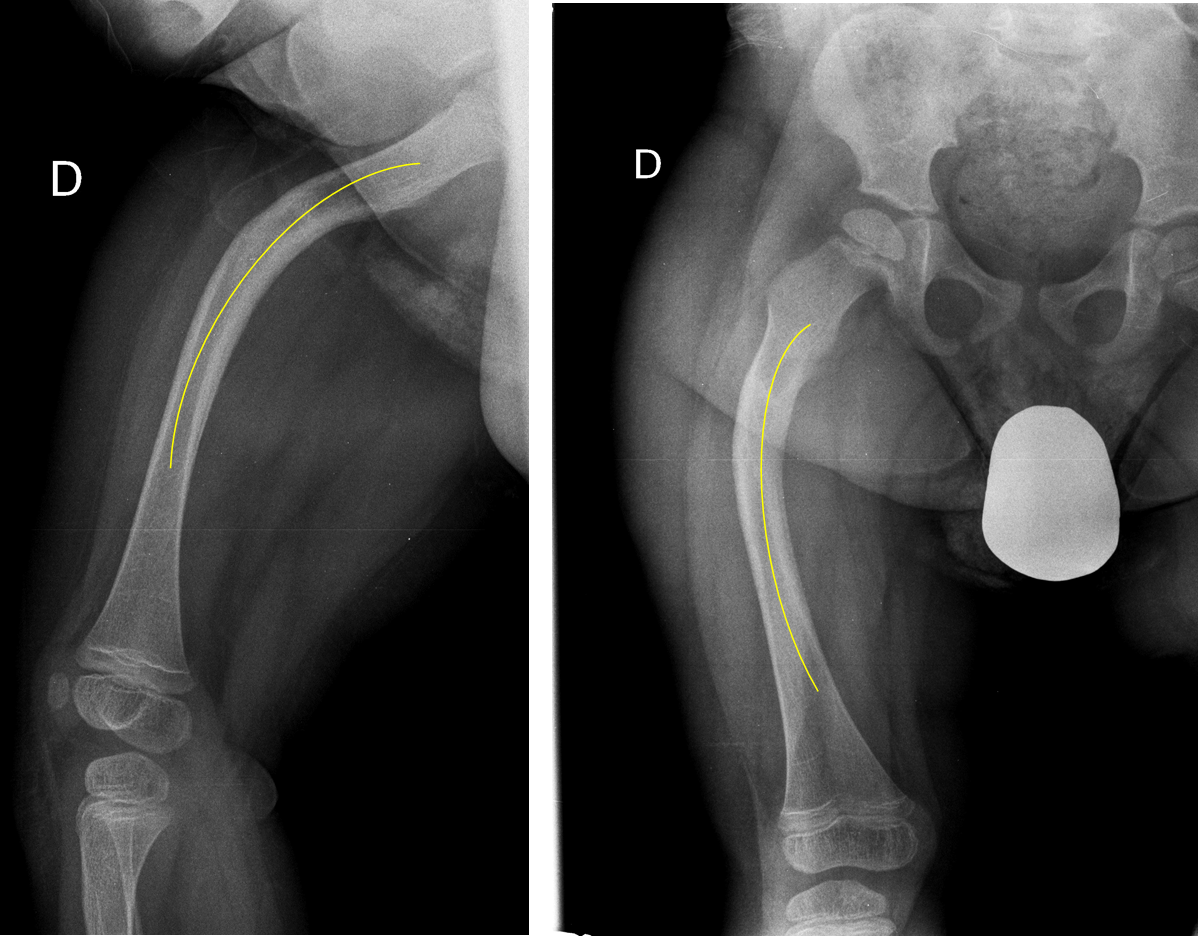
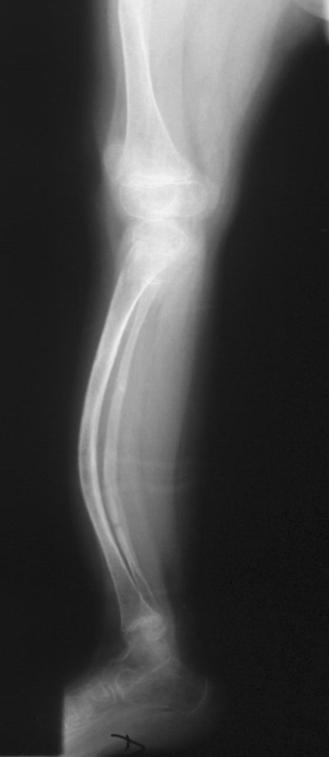
Deformities of the lower extremities are common in people with OI. Most patients display typical patterns of curvature: femur anterolaterally (outwards and towards the front, as in Figure 9), and tibia bowing anteriorly (a deformity popularly known as ‘bow leggedness’) (Figure 10).
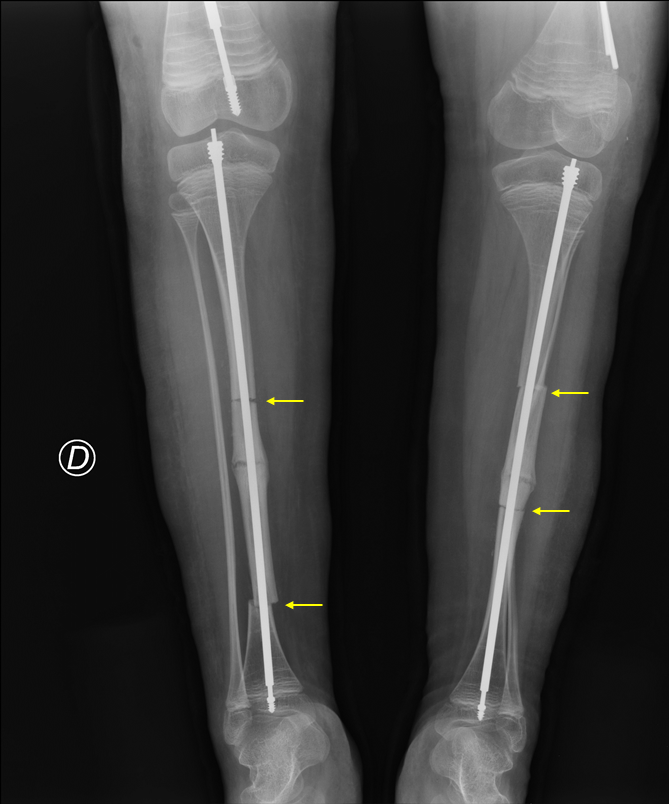
The deformities and curvature of the lower extremities modify the mechanical axis of the bone and the force that the body does on the deformed bone, making it much easier for fractures to occur. Sometimes, the deformity is so extreme that it may prevent the person from standing and walking. We must treat the malformations of the lower limbs considering the patient's age and degree of mobility (usually, they do not start treatment until they have learned to walk), the degree of deformity, and the number of fractures suffered. The most frequently used surgical technique is to make some cuts in the bone (osteotomy) at the points of maximum flexion and then align the bone with an intramedullary rod. This device provides more durability to the bone and helps maintain a correct position, reducing the risk of new fractures (Figure 11). A straight bone with a rod in its interior bears the body weight more safely than a curved bone without a supporting rod.