Osteogenesis imperfecta

1.1. Vertebral fractures
Vertebral fractures are relatively frequent in OI and occur in all the forms of the disease. They are generally the result of too much force being placed upon weak vertebrae, which become compressed and deformed. This force may be the consequence of a traumatism, which causes an acute fracture and the sudden appearance of pain. In severe cases, which are less common, the vertebral body may shift towards the spinal canal, compressing the marrow and causing neurological problems. Sometimes the vertebral body is progressively compressed by repeated microfractures, causing the patient chronic pain but with no other symptoms. As a result, it may only be discovered with routine x-ray.
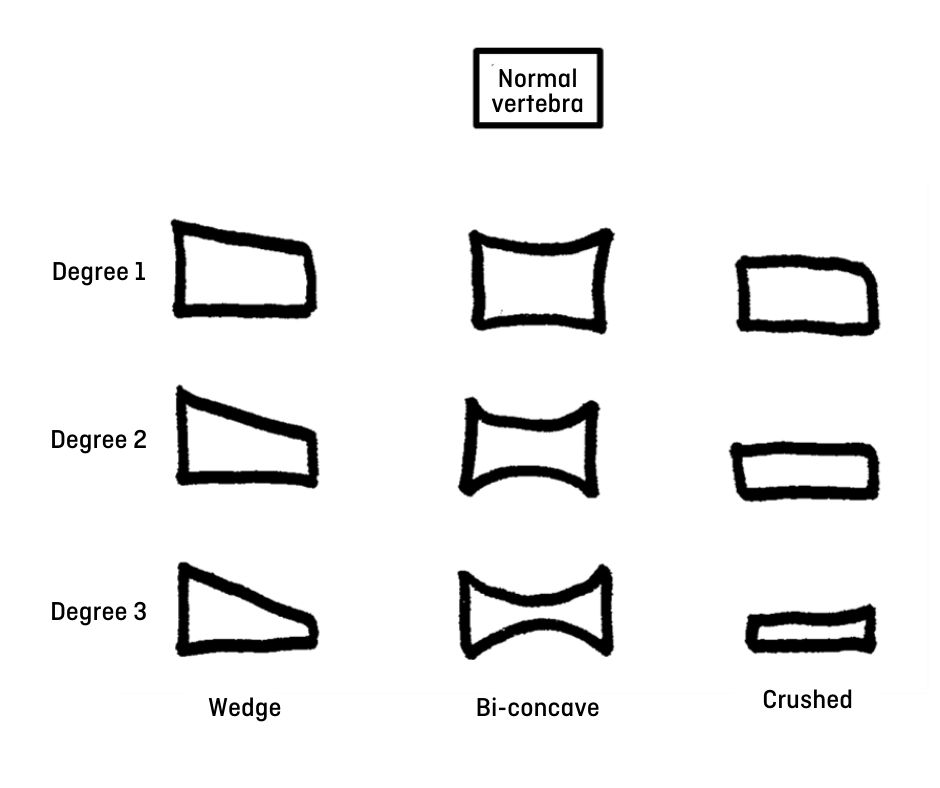
Most of vertebral fractures in OI are produced in the thoracic and lumbar vertebrae. Based on what shape adquires the vertebral body after the fracture, there different types of fractures (Figure 2):
- When the anterior part of the vertebrae is compressed, it may take the shape of a wedge, which may be more or less pronounced.
- On certain occasions, the central part of the vertebral body may collapse, taking a bi-concave form.
- Finally, the entire vertebral body may collapse, creating what is known as a crushed vertebra.
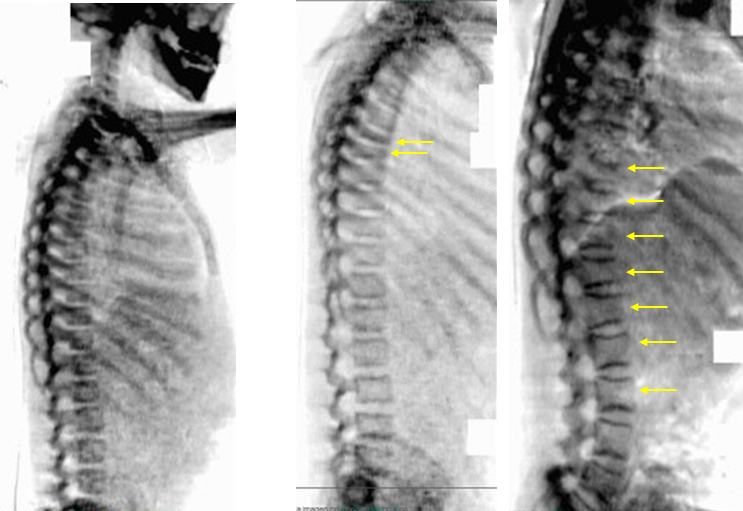
One of the key differences between children and adults is their ability to remodel the vertebral body after a fracture, which helps them go back (almost entirely) to their original shape and size (Figure 3). This remodeling capacity increases in children treated with bisphosphonates. For this reason, it is important to detect vertebral fractures early in childhood, this way we will be able to do a good follow-up and offer a treatment before the bones stop growing.

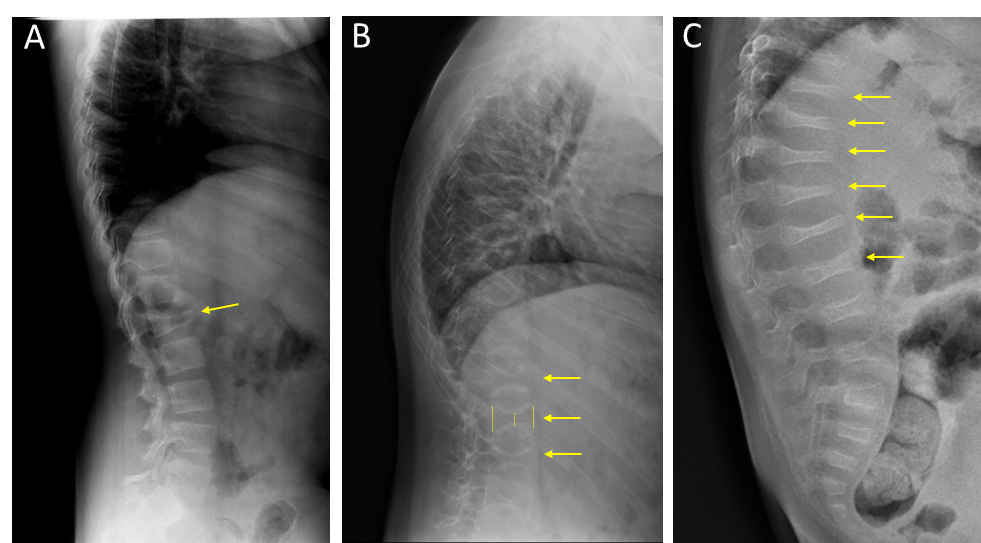
To diagnose vertebral fractures, it is necessary to obtain an X-ray of the spine, preferably with a lateral projection (Figure 4). Sometimes a CAT scan may also be required to have a more detailed picture of the bone. We can also perform an MRI to differentiate acute fractures from older fractures, or to assess whether the marrow is damaged. Nowadays, with some bone densitometry devices we can see a lateral projection of the column, which allows to assess the morphology of the vertebrae emitting less radiation than X-rays (Figure 5).
The presence of vertebral fractures may lead to column deformities (kyphosis, scoliosis), as we will explain later in this chapter, and also to the presence of chronic back pain in children and adults with OI.
The treatment of vertebral fractures needs to be specific for each patient, and for this we need to consider pain, degree and type of deformity and risk of neurological damage. In most cases, the pain can be controlled with a short period of rest and analgesics. In some mild cases of OI, the use of a corset may help to control the pressure on the ribs and prevent fractures and deformities in the rib cage. Finally, we can use surgery to manage vertebral fractures in OI, usually in adults.