Osteogenesis imperfecta

1.2. Scoliosis and kyphosis
Column deviations are relatively frequent in patients with OI. Depending on the direction of the deviation, we talk about:
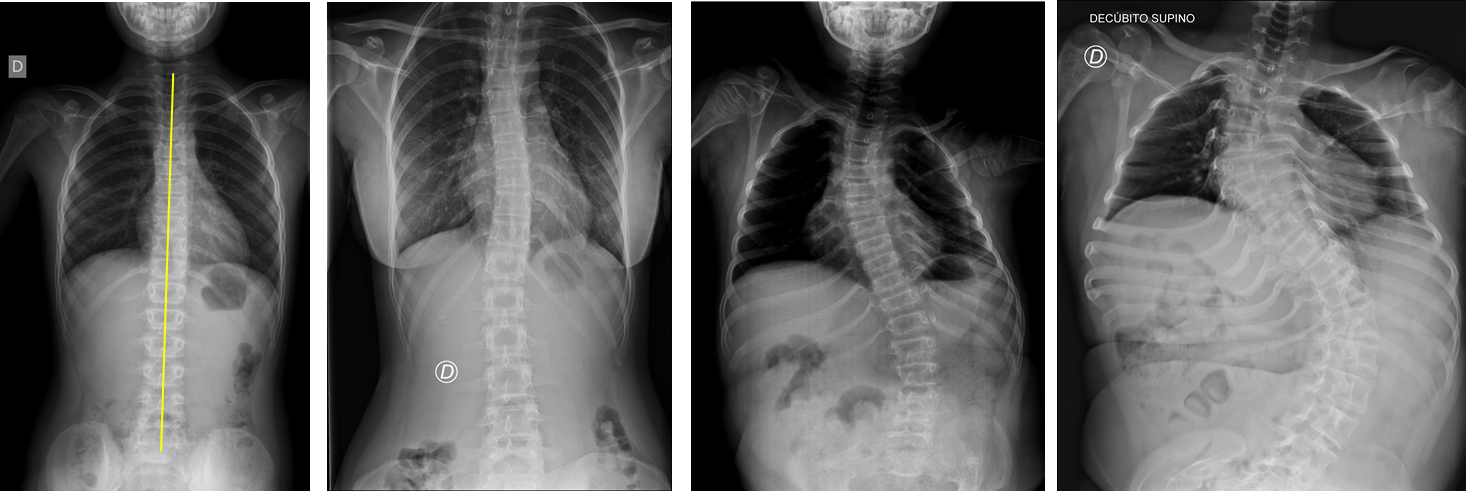
- Scoliosis: Under normal conditions, when viewed from the front or back the spine must form a straight line. In scoliosis, however, the column is twists and curves to the side, forming an S or a C (Figure 6).
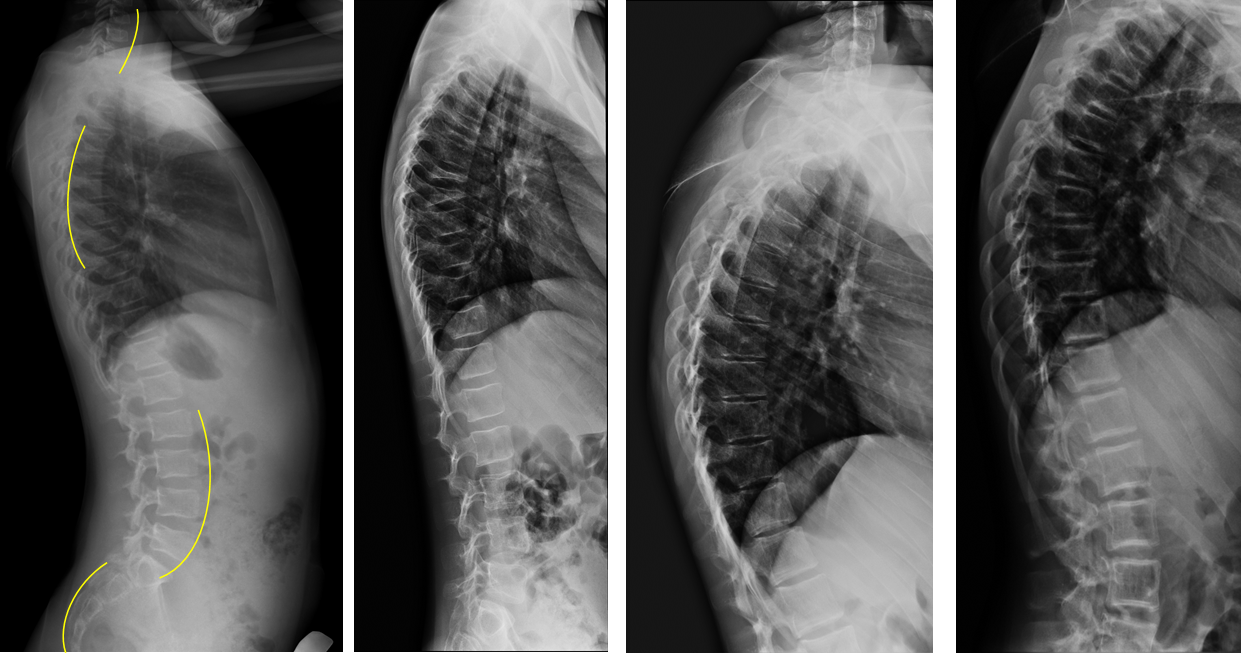
- Kyphosis: When viewed from the side, the spine has some curves: 2 convex curves, known as kyphosis (at the dorsal and sacral levels) and two inward concave curves, called lordosis (at the cervical and lumbar levels) (Figure 7). There is a pathological kyphosis when this curvature is too pronounced and the body twists forwards, sometimes creating a hunchback (Figure 7).
Between 39% to 80% of people with OI have some sort of scoliosis. Scoliosis generally appears at age 6 (although it can appear earlier) and it can progress rapidly, especially during the years that correspond to the peak growth, but it also progresses in adults. Some studies have found a relationship between scoliosis and low bone mass, proving that cases of OI leading to scoliosis show worse densitometry results than those that do not lead to scoliosis. Likewise, scoliosis is more common in severe forms of OI than it is in milder forms.
The origin of scoliosis in some patients with OI is still a matter of some controversy and may include factors such as the presence of fractures and deformities in the vertebrae, ligamentous laxity, weaker vertebral muscles and length differences between the lower limbs.
Apart from the discomfort and physical deformity produced by scoliosis, it also alters the morphology of the thoracic cage and may compromise lung capacity, especially in those cases with a highly pronounced curvature.
It is less frequent than scoliosis, but OI patients may also develop pathological kyphosis. It may appear alone or in combination with scoliosis, a phenomenon known as kyphoscoliosis. Kyphosis usually appears in relation to vertebral fractures, especially when the vertebral body acquires a wedge shape. It is usually noted in the thoracic spine, but may also appear in the lumbar or cervical spine.
Children affected by OI should be examined annually for clinical signs of spine deformities, and if these do appear, we should increase controls, especially during the years of maximum growth when it can progress more quickly. The treatment of scoliosis and kyphosis in OI patients is usually more difficult because of the poor quality of the bone and the rigidity of the deformity. Corsets (used in patients with scoliosis who do not have OI) have not shown to impair curvature progression in patients with OI. Also, corsets may induce rib fracture and/or produce deformity of the thoracic cage, so they are not commonly used in OI. Surgical fusion of the column — joining several vertebrae with metal plates or rods — may be an option in some patients with severe or progressive scoliosis or kyphosis. This is an aggressive surgical procedure that may have complications such as infection, fracture of vertebrae and ribs, pain and neurological problems. For this reason, each patient must be individually evaluated: degree of curvature and rate of progression, rigidity of the curve, impairment of pulmonary capacity, and so on. Ideally, the OI patient that is going to undergo spine surgery should be treated beforehand with bisphosphonates in order to improve the quality and durability of the bones.