Epidermolysis bullosa

1. The skin and its affectation in EB
The skin is the most extensive organ of the body and it acts mainly as a protection barrier isolating the organism of the surrounding medium. It also communicates the body with the environment and it is one of the main sensory organs of our body, as it has a massive amount of nerve endings that collect information about the temperature, pressure, pain and touch. Furthermore, the skin plays a crucial role in the absorption and excretion of substances, including sweat, and is also responsible for synthesising 90% of the essential vitamin D required for maintaining our health. This process occurs in the skin, as it needs ultraviolet radiation from the sun.
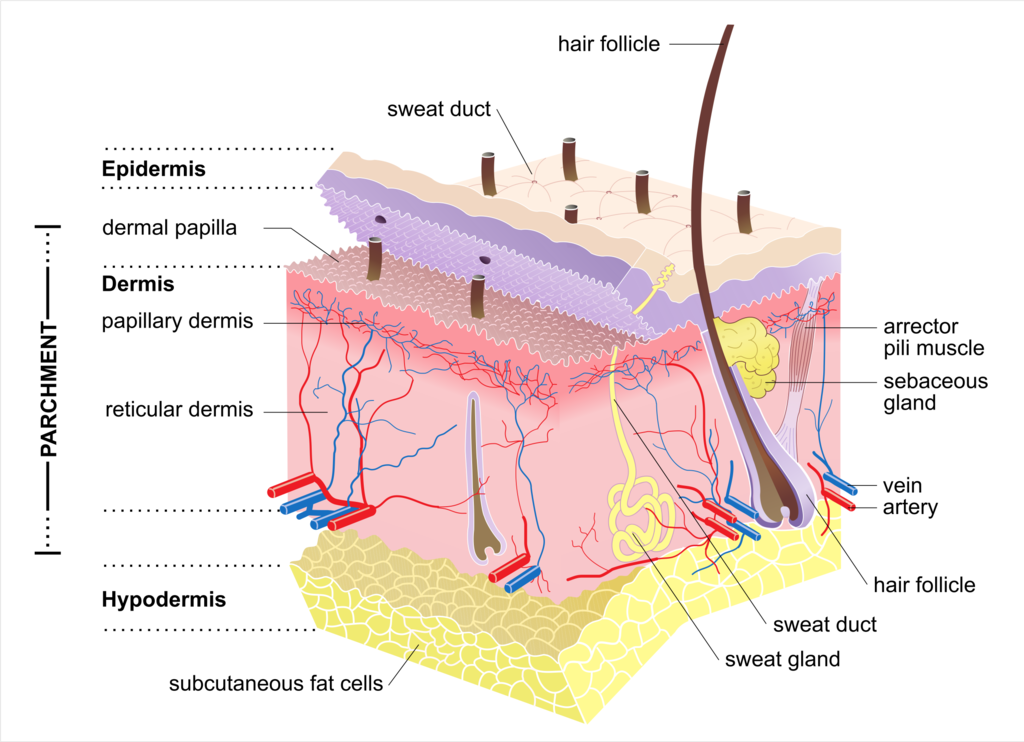
The skin is formed by an external layer called the epidermis and a deeper layer called the dermis. Both are separated by the basal lamina, which keeps these two layers together. Under the dermis, we find the hypodermis or subcutaneous cellular tissue, formed by adipose tissue or fat and muscular layer, right underneath (Figure 1).
The epidermis is made up mainly of cells called keratinocytes. It also contains other types of cells like the Langerhans cells, which will give immunologic protection, and melanocytes, melanin segregating cells responsible for skin pigmentation. The epidermis grows constantly from the base in a cycle that lasts approximately 4 weeks. The new cells are formed in the base of the epidermis and migrate to a more superficial stratum, where they will end up detaching in a process called peeling or desquamation.
The dermis is characterised by its abundance of collagen fibres and other components that give the skin its consistency and elasticity. The dermis is generally thicker than the epidermis: In it, we can find the so-called pilosebaceous units formed by the glands, the hair and the erector muscle. The dermis also contains blood vessels and nerve endings that enable the sense of touch and provide heat, cold, pressure and pain sensitivity.
In epidermolysis bullosa (EB), some of the components of the skin are altered, giving rise to the different manifestations of the disease. If the concrete within a wall is removed or insufficiently binds the bricks together, there is a higher likelihood that the wall could collapse even from a minor impact. This is an analogy to EB. The skin can be defined as a wall, cells (or keratinocytes) are its bricks, and proteins are the concrete. When the proteins are missing or have a different structure that makes them non-functional, the integrity of the skin is compromised, and its layers (epidermis and dermis) are damaged with the slightest touch or trauma, forming blisters.
The most characteristic feature of EB is the extreme fragility of the skin and the mucous membranes, as well as the appearance of blisters caused by hits, touches or even spontaneously. The fragility stems from mutated skin proteins: the body either generates a reduced quantity of these proteins or none at all, rendering them incapable of fulfilling their role in maintaining skin integrity and elasticity.
EB is clinically very heterogeneous and its severity varies a lot. Currently, more than 20 genes are associated with this disease. Pathogenic mutations (mutations that cause a disease or disorder) have been found in genes translated into collagens, laminins and integrins. These proteins are essential for skin integrity and resilience and, depending on what happens to each protein (absent, reduced, non-functional, etc.) and on which skin layer they are located, the disease has different grades of severity.
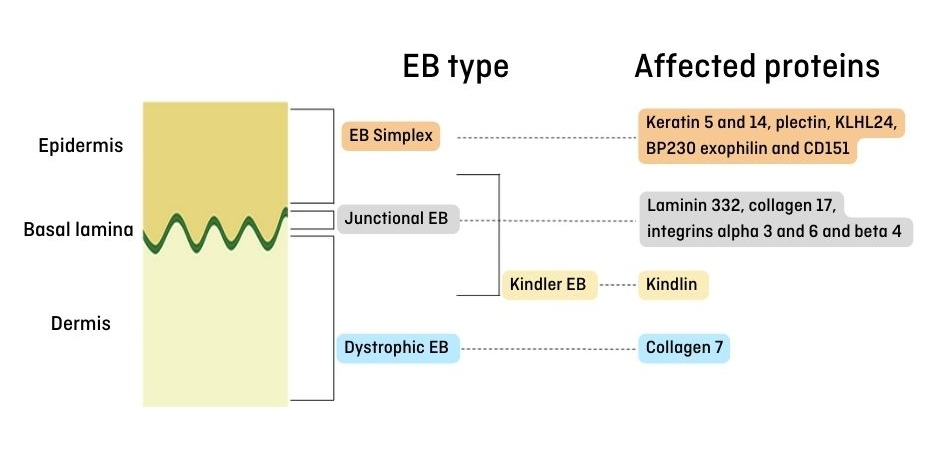
In an introductory way, EB is classified into four main types: simple, junctural, dystrophic and Kindler’s. In each type of EB, there are one or more affected proteins. In Figure 2, we show the location of the different skin proteins affected in epidermolysis bullosa.
Epidermolysis bullosa is manifested in all ethnic groups and affects both sexes alike. It has been estimated that the worldwide incidence of carrier individuals (those who have an EB-related mutation in their genome) is 1 out of 227 people. In Spain, it is estimated that the incidence (number of new births per year) is around 5 cases out of 100,000 newborns. As for the prevalence (number of people who have the disease), there are approximately 1,000 people with EB in Spain (2.4 people per 100,000 inhabitants).