Juvenile dermatomyositis

3. Gastrointestinal manifestations
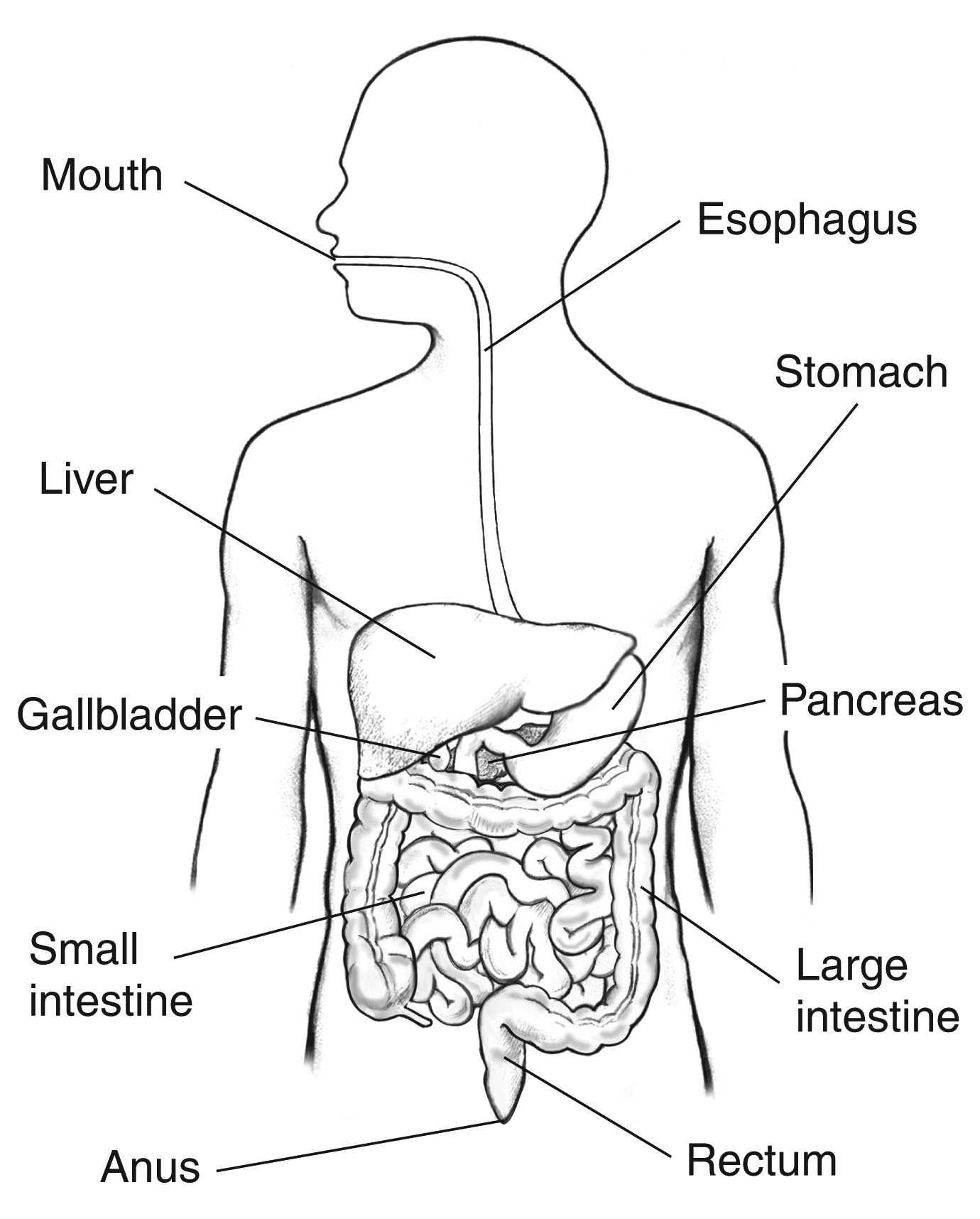
The digestive system is made up of the mouth, esophagus, stomach, small intestine, large intestine and rectum (which is the final part of the large intestine). It begins in the mouth, which is where the food enters our organism, is crushed and mixed with saliva to form the alimentary bolus. After chewing, it is swallowed, passing through the pharynx to the esophagus. The esophagus is the tube that connects the mouth with the stomach, and by means of contractions it moves the food. It also has a system of non-return of the food consisting of a circular muscle at the beginning and another at the end, which contract after the passage of the food bolus, preventing it from going backwards. They are called sphincters. In the stomach, the acid digestion begins thanks to the gastric juice and then the food passes to the small and large intestine by means of movements of the muscle of the intestinal walls. The food is pushed thanks to the work of the muscles of the gastrointestinal tract throughout its journey.
The digestive tract has several layers. The innermost ones, which contact the food, form the digestive mucosa, composed of cells, glands and transport systems to absorb the food. The outer layer is formed by smooth muscle, whose purpose is to propel the food and mix it with the different products secreted by the digestive system (gastric juice, bile...).
In juvenile dermatomyositis there may be gastrointestinal involvement due to weakness of the musculature involved in the process of food propulsion and/or inflammation of the blood vessels that nourish the digestive tract.
- Oropharyngeal dysphagia: Difficulty in the propulsion of food at the level of the mouth and pharynx is known as oropharyngeal dysphagia. It is common for patients to present impaired swallowing at diagnosis of the disease, although it is not so common for this alteration to be associated with the presence of symptoms (coughing with ingestion due to the passage of contents into the airway, choking, etc.).
- Gastroesophageal reflux: It occurs when the acid content of the stomach ascends through the esophagus, either because there is a weakness of the anti-reflux muscles (sphincters) or because gastric emptying is slowed down. It may be asymptomatic or may produce chest pain in the sternal area and/or passage of food content into the airway associated or not with symptoms.
- Intestinal ischemia with/without perforation: this is the most severe gastrointestinal manifestation of the disease. It may be caused by inflammation of the blood vessels responsible for nourishing the walls of the digestive tract. It is usually associated with severe abdominal pain, "board abdomen", fever and laboratory abnormalities.
- Liver involvement in the context of juvenile dermatomyositis is rare.
To evaluate gastrointestinal involvement, different diagnostic tests can be performed depending on clinical suspicion.
- Videofluoroscopy: This is a radiological exploration of low irradiation that allows to study in real time how the food (in this case together with a contrast) is propelled from the mouth to the esophagus. It allows us to evaluate the function of the tongue, palate, larynx... It allows us to evaluate the efficacy and safety of swallowing and to obtain data on its biomechanics.
- Barium transit: It is a technique that allows us to evaluate the shape and functionality of the gastrointestinal tract, both proximally (esophagus, stomach) and distally (small and large intestine). It allows to detect different gastrointestinal alterations such as abnormal movements or esophageal dilatations, ulcerative lesions, areas of stenosis...
- Depending on the clinical suspicion, we have different imaging tests such as ultrasound, computed tomography, entero-resonance or angio-resonance, which allow a detailed evaluation of the gastrointestinal tract.
- Upper gastrointestinal endoscopy: This allows direct visualization of the esophagus and stomach and evaluation of the presence of lesions through a camera attached to a flexible tube. To perform it, the child must be sedated so that the test does not bother him/her.
Warning signs:
- Abdominal pain or mild abdominal discomfort is a common symptom in children. However, if abdominal pain becomes very persistent, intense or disabling, it should be considered a warning sign and be evaluated by the physician.
- Blood in the stool, persistent diarrhea.
- Cough with ingestion.