Juvenile dermatomyositis

1. Respiratory manifestations
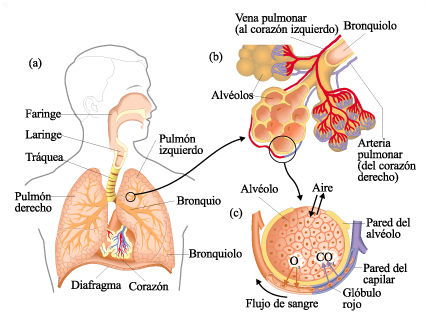
The lungs are formed by an elastic tissue, which expands with respiration. In this tissue are the alveoli, which is where gas exchange takes place, oxygen is absorbed and carbon dioxide is eliminated. The oxygen diffuses to the small blood vessels (capillaries) that surround the alveoli and from there carry this oxygen-filled blood to the heart, which distributes it to the organism. The tissue containing the alveoli is called the pulmonary interstitium.
The air reaches the alveoli through the trachea, which divides into bronchi that subdivide into bronchioles until the alveoli are found in the most distal zone. For oxygen to reach the alveolar capillaries, the airways must remain clean, the tissue must be sufficiently flexible and there must be no damaged areas between the alveoli and the alveolar capillaries to hinder its passage.
In juvenile dermatomyositis, lung tissue may be affected in 8-10% of children. In many cases there are no symptoms, but in some cases there may be significant inflammation of the lung tissue, known as interstitial pneumopathy. The onset of symptoms is highly variable, ranging from cases in which the onset is rapid with fever, cough and respiratory distress with the appearance of radiological changes within a few days, to cases in which only changes are detected in functional tests (i.e. those that measure how air enters and leaves the lungs or how it diffuses) without the child having any symptoms.
Although it is not known why some patients develop pulmonary involvement and others do not, we do know that there are some markers (autoantibodies) that are associated with a higher frequency of respiratory symptoms.
The evaluation of pulmonary involvement is first performed by looking for symptoms or signs suggestive of pulmonary involvement: cough, expectoration, shortness of breath, elevated respiratory rate or the detection of abnormal sounds on lung auscultation. In addition, a series of explorations should be performed to complete the study:
1. Respiratory function tests: These tests evaluate how the child breathes and how air diffuses into the lung. Different devices called spirometers, plethysmographs or carbon monoxide diffusion meters (DLCO) are used for this purpose. During the test the child must breathe through a mouthpiece or mask with varying intensity throughout the test. It is a painless test, which does not pose any risk to the child, but it requires the child's cooperation, so if the patient is very young it cannot be performed. In juvenile dermatomyositis the functional tests may be altered by involvement of the lung itself or by weakness of the muscles that collaborate in breathing.

2. Imaging tests: They complement physical examination and respiratory functional tests. The most frequent is the simple chest X-ray. Sometimes it is necessary to perform a computed tomography (CT).