Osteogenesis imperfecta

2.3. Anomalies in the base of the skull
The most common anomalies of the skull base in individuals with OI are platybasia, basilar impression, and basilar invagination.
Platybasia refers to an abnormality in the shape of the skull where the lower part of the skull base becomes flattened. This condition has been observed in various disorders. In OI, it is believed that the weight of the brain leads to microfractures and/or deformities in the bones of the skull base, resulting in flattening.
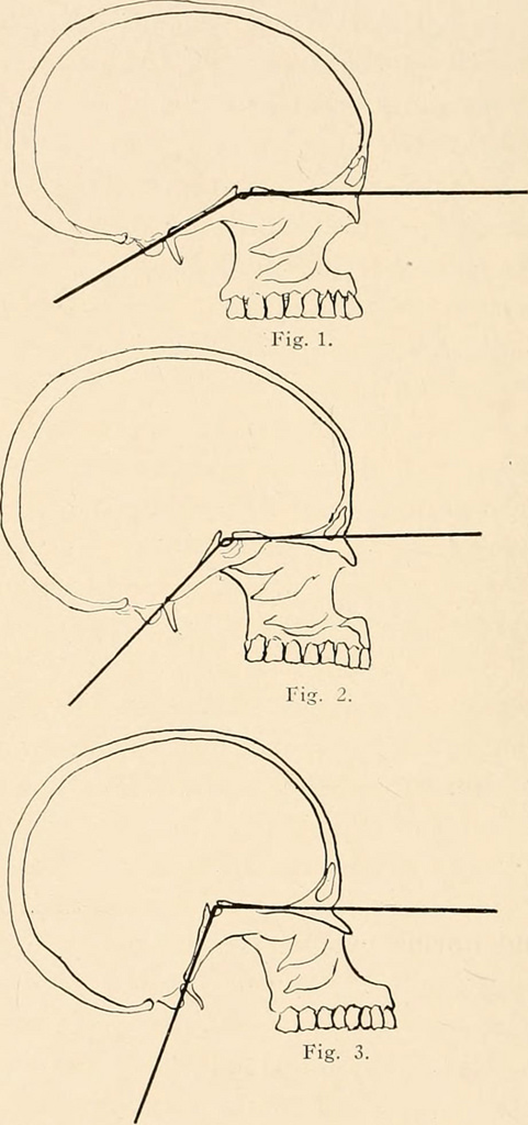
Platybasia itself does not typically cause any symptoms and is primarily a morphological alteration that can be detected through lateral skull imaging. Radiologists can analyze a skull radiograph, identify different reference points on the skull base, and draw lines to determine the angle of intersection. This angle assessment helps in diagnosing the presence or absence of platybasia (Figure 6).
In basilar impression and basilar invagination, the skull base descends relative to the upper cervical vertebrae, resembling a sinking of the skull while the spine moves inward towards it. To illustrate this, imagine the skull and spine as a lollipop, with the candy (skull) sinking down on the stick (spine). Consequently, individuals with these conditions may appear to have a shorter neck. Similar to platybasia, diagnosing basilar impression and invagination often involves evaluating specific lines and angles. One point of reference for these measurements is the odontoid process of the axis or second vertebra, which is a protrusion that can be identified on imaging. If the odontoid process is above the opening of the skull base (foramen magnum), it is known as basilar invagination. On the other hand, if the odontoid process is above the lower edges of the skull without entering the skull opening, it is referred to as basilar impression. The spinal cord, responsible for transmitting signals between the brain and the body, passes through the skull opening. In cases of basilar invagination, the protrusion of the vertebrae into this opening can compress the spinal cord and the exiting nerves.
While not all patients with basilar invagination experience symptoms, nerve compression can lead to progressive disturbances that may pose a threat to the patient's life. Common symptoms include posterior headaches, hand weakness or numbness, abnormal eye movements, changes in voice tone, difficulty swallowing, sleep apnea, dizziness, and more.
Although platybasia can coexist with basilar impression and invagination, it can also occur independently and may not require treatment. However, when symptomatic basilar invagination necessitates intervention, surgical decompression may be necessary. This can be achieved through external traction using a halo device attached to the head, which pulls it upwards, or through surgical techniques involving the removal of the compressing odontoid process. Various surgical approaches have been described, but due to the proximity to critical structures such as the brain, spinal cord, and major nerves, surgical complications should not be underestimated. The choice of surgical technique and timing should be individualised for each patient in consultation with a neurosurgeon and other relevant specialists. Additionally, cranial and spinal stabilisation using metallic devices is often performed during decompression to prevent further sinking of the skull onto the spine.