Osteogenesis imperfecta

2. The lungs in OI
The respiratory system consists of the airways and the lungs. Its main task is breathing, which is to bring oxygen into the body and remove carbon dioxide that has been produced during metabolism. The lungs are protected by a bony cage (the rib cage), which is formed by the sternum bone, ribs and spine.
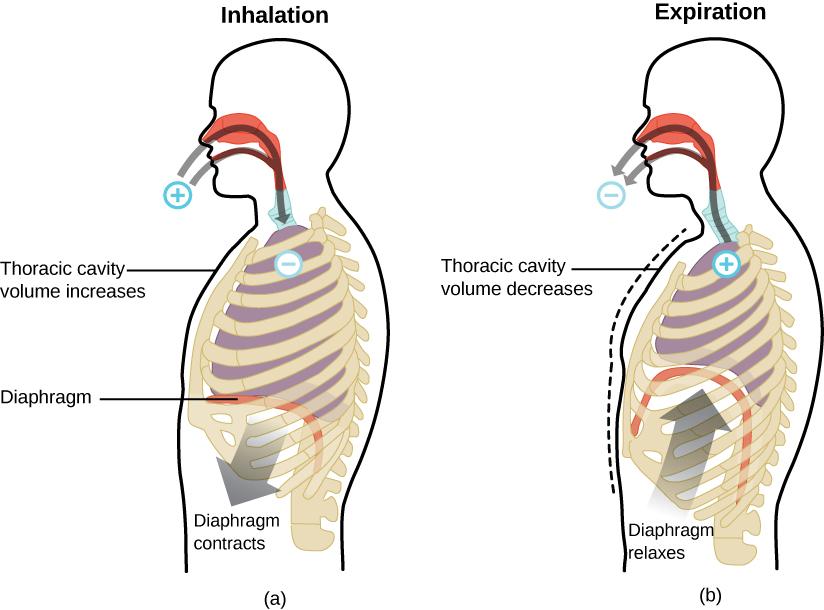
Breathing consists of an inspiration phase (air in) and an expiration phase (air out). During inspiration, air enters through the nose and/or mouth. From there it is drawn into the throat (pharynx) and then into the larynx (where the vocal cords are located). It then passes into the trachea, which divides into two bronchi, each of which leads to a lung. The lung is like a sponge, made up of multiple sacs called alveoli. It is in the alveoli of the lungs that gas exchange takes place: oxygen from the air passes into the blood and is transported to all the cells of the body, while carbon dioxide passes from the blood into the lung and is eliminated through the same airways to the outside of the body with exhalation.
Because oxygen is the fuel needed by all cells in the human body, obtaining sufficient oxygen is important for maintaining good health. Respiratory manifestations in OI are frequent and often progressive, being one of the main reasons for decreased quality and length of life, especially in moderate and severe forms.
The main respiratory problems in OI may be due to:
- Alteration of the rib cage: the presence of scoliosis, kyphosis, vertebral or rib fractures or anomalies at the level of the sternum (pectus scavatum, pectus carinatum) can produce an alteration in the shape and capacity of the rib cage that hinders the expansion of the lungs inside it. This leads to a reduced ability to move air with each breath, resulting in less gas exchange. This results in shortness of breath, shortness of breath and in severe cases respiratory failure may occur in which the patient needs oxygen or machine support to be able to breathe (artificial respiration). In addition, if the lung cannot expand properly, there may be less ventilated areas where secretions accumulate, facilitating the development of respiratory infections and pneumonia.
- Alteration of the pulmonary connective tissue: in mild forms of OI, despite not having deformities in the rib cage, it has also been shown that the lungs may be affected. Type I collagen is found in abundance in the pulmonary connective tissue, especially around the alveoli, which would explain why forms of OI with collagen alteration present dysfunction at the level of this pulmonary tissue, thus hindering correct gas exchange.
- Abdominal influence: the smaller size and the presence of deformities in the spine mean that the abdominal space is smaller, which produces greater pressure on the lungs, making it difficult for them to expand properly. This greater abdominal pressure can also favour the reflux of gastric juices that can pass into the airway (aspiration), leading to a greater risk of infection and symptoms of coughing, wheezing and shortness of breath (asthma symptoms). This can be aggravated by constipation, which is also common in OI.
The presence of nocturnal obstructive sleep apnoea has also been associated with OI. Sleep apnoea is characterised by episodes of shallow breathing and/or breathing pauses during sleep, which cause insufficient respiratory rate and result in fragmentation of sleep and therefore rest, leading to fatigue and daytime sleepiness. It is more frequent in moderate-severe forms of OI and/or with thoracic and cranial deformities and in overweight patients.
In addition, respiratory diseases common in the general population also occur in OI, but the effects of these are often magnified in OI patients.
Imaging tests (X-rays, lung CT, etc.), functional respiratory studies such as spirometry or sleep studies can be used to assess lung involvement.
Treatments include inhaled drugs (bronchodilators, corticosteroids, etc.), antibiotics for infections, respiratory physiotherapy (manual or with airway clearance devices). Patients with sleep apnoea may require special devices to increase airway pressure and improve breathing during sleep.