Epidermolysis bullosa

4. Preparation of the wound bed
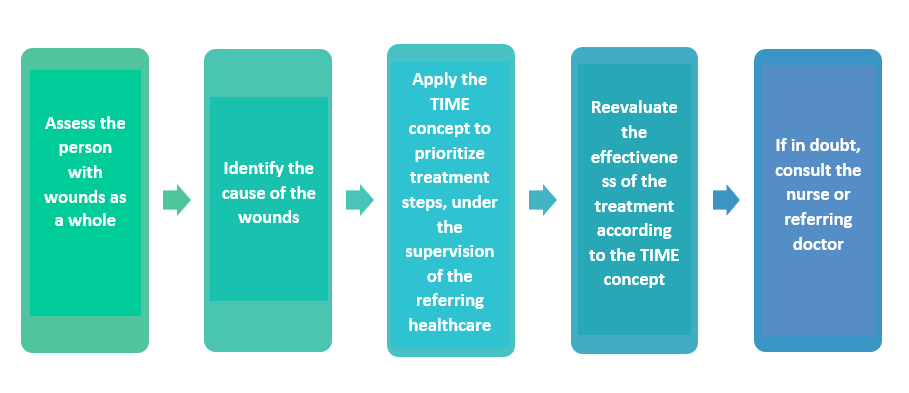
If we want to achieve a better wound cicatrization, we need to remove the obstacles in the way, favouring the process of natural cicatrization. The “TIME” concept is presented as an orderly scheme which might guide us in the tackling of chronic wounds (Figure 3). This scheme should not be understood as something lineal, but as something that can help un assess what the wound needs at each moment and adapt to its needs when making our daily decisions. These wound treatment principles are appliable to wounds in patients with EB, especially in chronic wounds.
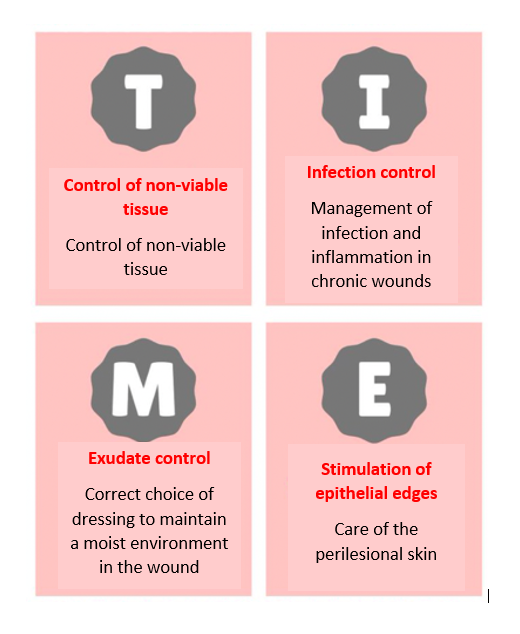
The main components in wound treatment, following the acronym “TIME”, are the following:
- Tissue – Control of the non-viable tissue.
The non-viable tissue is non-healthy tissue present in the wounds which hinders or prevents the natural cicatrization process. It can be dry and hard (necrotic plate) or humid and soft (sloughed tissue and/or fibrin), of different colour shades.
- Cleaning is the first step to remove the waste or non-viable tissues from the wound (dry skin, scabs, slough or mucous tissue, etc.). In cases where there are many debris that cannot be removed by cleaning, debridement is necessary. An adequate control of non-viable tissue can help us to minimize the presence of microorganisms and the risk of infection in the wound.
- Crusted wounds are common in people with EB, especially wounds that are left uncovered because they are in complex locations (for example: nose, ears, etc.). Scabs can delay healing and promote infection, so whenever possible they should be removed with: moisturizers such as vaseline (they will make it softer and easier to remove the scabs in the next treatment) and hydrogel or dressings suitable for autolytic debridement (this concept will be explained in a later section). We should not remove the scabs by strongly pulling on them but encourage them to come off on their own or, in any case, trim the parts that are detached from the skin with scissors.
- Some wounds have slough, which is a mucous layer, more or less sticky (soft or hard depending on the amount of water) and of different colours (usually whitish, greyish or yellowish). Slough are waste tissues that, just like scabs, impair healing and must be removed with debridement techniques that we will see later.
- Infection – Control of the inflammation and infection.
The infection must be evaluated by your reference professional team and, in case of needing any treatment other than intense cleaning and debridement, it should always be under medical indication. Likewise, before starting pharmacological treatments there are disinfectants (polyhexanide solutions, sodium hypochlorite, etc.) which might help reduce the number of microorganisms in the wounds. Since infections can be caused by different types of microorganisms (bacteria, virus, fungus, parasites, etc.), its treatment might vary in each case. Therefore, antibiotics are not always required and can even be counterproductive in certain cases.Sometimes it may be necessary to culture the wound exudate using a smear (a sample is taken from the wound by rubbing it with a cotton swab) to identify the main agent causing the infection. The main local antimicrobial products are:
- Creams. It is not recommended the daily use of antibiotic creams, as its effect is limited as it is applied at a local level and there is a risk of developing allergic reactions and resistance to microbes, with them becoming accustomed to its effects and leaving the cream useless. Likewise, applying creams can interfere with the adequate management of the wound’s humidity.
- Dressings. There are dressings with antimicrobials like silver which, although they are not specific antibiotics for a particular type of microorganism, reduce the bacterial load, in other words, the number of living microorganisms in the wound. However, silver must be used with precaution during less than 14 days (never in children under 1 month old), as it can produce adverse reactions. On the other hand, there aremesh dressings which retain microorganisms and help eliminate them, without being antimicrobial per se.
- Solutions or gels. There are cleaning solutions and gels disinfectant or decontaminants, which help cleaning deeply the wound and at the same time disinfect and end with the microorganisms. However, we must use those solutions with disinfectants apt for open wounds, as there are some common disinfectants (for example, chlorhexidine or povidone iodine) which might be harmful when applied directly and repetitively on open wounds.
- Moisture – Control of the exudate and the moisture imbalance.
As previously mentioned, it is advisable to have a humid environment on the wound to promote its cicatrization. However, we must control the humidity so that its excess does not damage the edges and difficult the wound’s healing. At this point, it is recommended to choose a dressing that adequately manages the wound’s exudate, spacing as much as possible the need to change dressings and bandages. Wounds which exudate a lot might need super absorbent dressings, which should always be used over a primary non-adhesive dressing.
- Edge – Evaluation and stimulation of the wound’s edges.
For the wound to progress successfully, the edges should not be thickened, inflamed, or damaged by moisture. A sign that the wound is developing correctly is that the edges are at the same height as the base of the wound (not raised or depressed), allowing new tissue to build up from the periphery of the wound to the centre. It is advisable to follow what is recommended in the previous paragraph, as well as to adequately monitor the surrounding skin, making sure that the dressings are well fixed to the wound and do not move (because they could create new wounds on the edges).
Recently, the letters “R” and “S” have been added to the acronym. The R refers to advanced research therapies and the S refers to socio-environmental aspects. This last component refers to the importance of assessing the context of each person who has one or more wounds, to choose the best care at all times with a global vision of the person. Although the nursing professional will be the one who tells you the type of cure that each wound needs at all times. It is important to keep this in mind when dealing with unforeseen changes in day-to-day life and to be able to continuously re-evaluate wounds when the expected healing does not occur. In case of any doubt, it is always necessary to consult with the reference nurse.