Kabuki syndrome

2. Neurological symptoms
Hypotonia
In Kabuki syndrome, neurological development is affected from the earliest stages of life. An early neurological manifestation is hypotonia (decreased muscle tone) with decreased osteo-tendon reflexes. Hypotonia manifests in the first days or months of life in the form of weak sucking and swallowing and hinders infant feeding. For this reason, some infants are fed by nasogastric tube and, to a lesser extent, by gastrostomy. Later on, it may favor psychomotor delay in some developmental steps such as sitting or walking.
Abdominal hypotonia can lead to constipation, inguinal hernias and cryptorchidism (failure of the testicles to descend into the scrotal pouches); axial hypotonia (of the muscles on the sides of the spine) can lead to spinal deviations (called scoliosis); hypotonia of the lower extremities can lead to dislocations in various joints: hips, knees or ankles.
Cranial growth
In neurology it is very important to assess cranial growth, by measuring the cranial perimeter and the growth curve with age, which guides us on an adequate brain growth.
Children with Kabuki syndrome often have decreased skull size, called microcephaly (low cranial growth). It can be an indirect sign of developmental delay and does not necessarily indicate other neurological problems or brain malformations, but it is important to measure over time to see the neurological evolution.
Seizures
Epileptic seizures are due to an abnormal and simultaneous discharge of a group of neurons, usually located in the cerebral cortex. They can be due to multiple causes: fever (febrile seizures), brain infections (such as meningitis or encephalitis), cranial trauma, dehydration, lack of oxygen (e.g. in cardiac arrhythmias), epilepsy, etc.
Thus, epilepsy is not synonymous with epileptic seizures. Epilepsy is defined as a chronic lesion of the brain (e.g. a brain malformation or a genetic disorder) that manifests itself in the form of epileptic seizures.To diagnose a child or adult with epilepsy, it is necessary that he/she has presented at least 2 epileptic seizures in the absence of a transient cause (e.g. fever, infection, trauma), and preferably that there are compatible alterations in the electroencephalogram.
Epilepsy has been described in kids with Kabuki syndrome but that does not mean that all children have epilepsy.
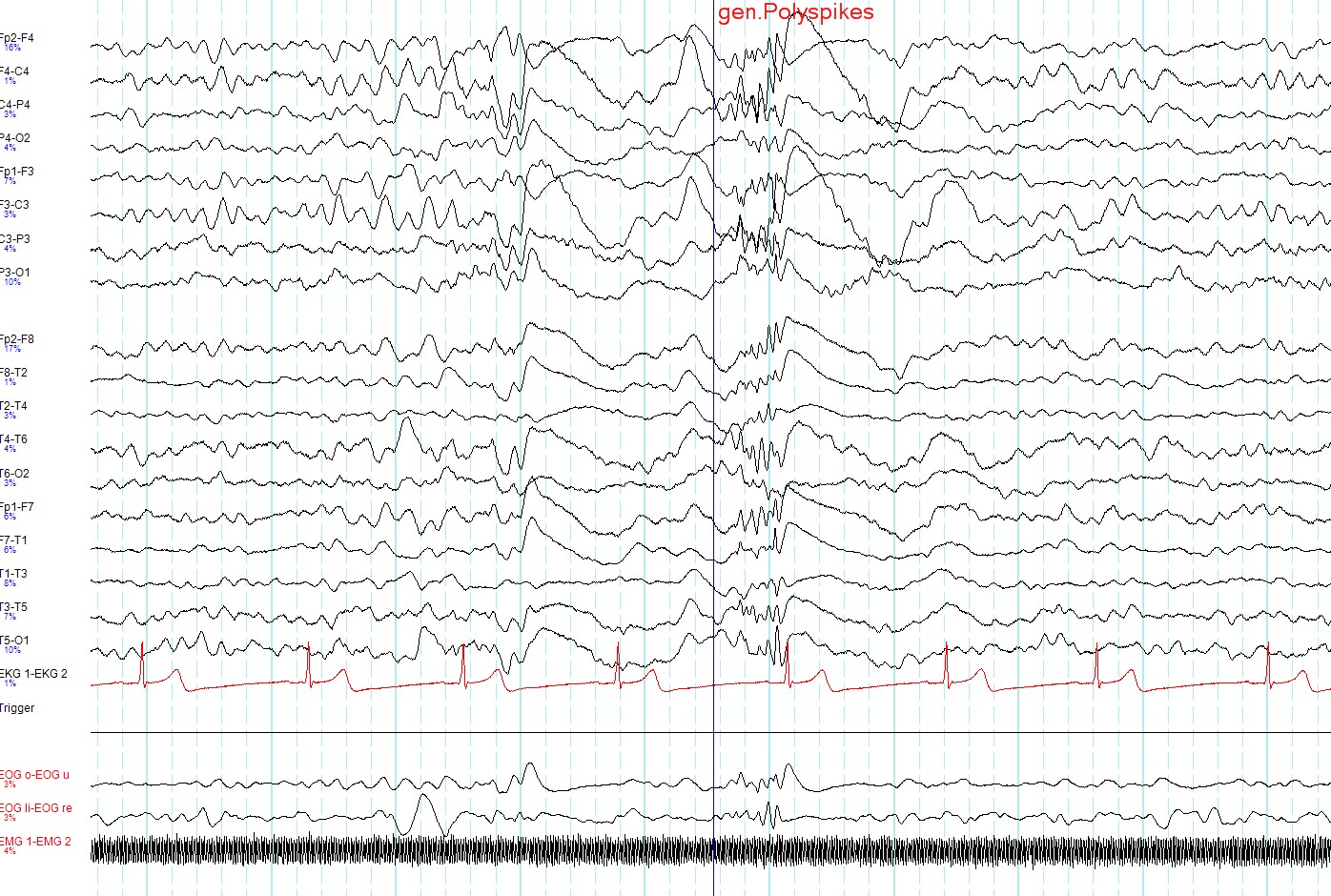
The diagnosis of an epileptic seizure is made by clinical history (the patient's symptomatology is fundamental) and is supported by the electroencephalogram or EEG.
The EEG is a recording of the electrical activity of neurons. There are external factors that favor the appearance of EEG abnormalities, which are systematically applied during recordings to optimize the performance of the test.
There are many different types of epileptic seizures, just as there are different types of EEG findings depending on the type of seizure presented by the patient, the underlying disease, the use of anti-epileptic medication...
Neurological development
From the cognitive point of view, one of the things that most concern parents of children with Kabuki syndrome is the intellectual deficit or disability. Intellectual deficit is a frequent manifestation and most children present with mild to moderate, some with severe degrees. Intelligence tests assessing IQ show great variability.
In general, there is a slowness in both speech and reasoning, so these are children who, with more time to perform activities, their performance improves greatly.