Kabuki syndrome

2.2. Secundary skeletal anomalies
2.2.1. kyphoscoliosis
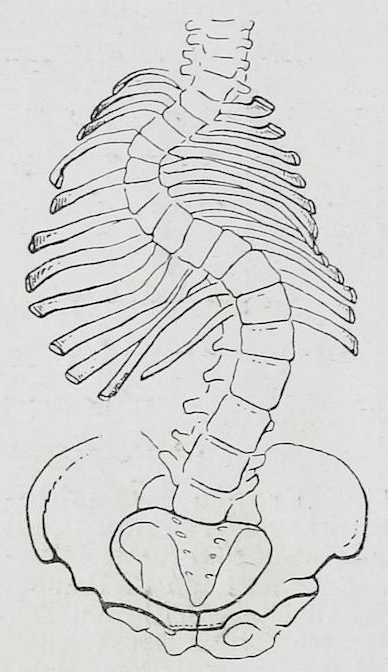
The spine should appear straight when viewed from the front or back. When it is tilted to one side, this is known as a scoliotic posture (for example, when sitting sideways). If this scoliotic posture persists over time, true scoliosis can develop, where the spine is not only tilted to one side but also has rotated vertebrae.
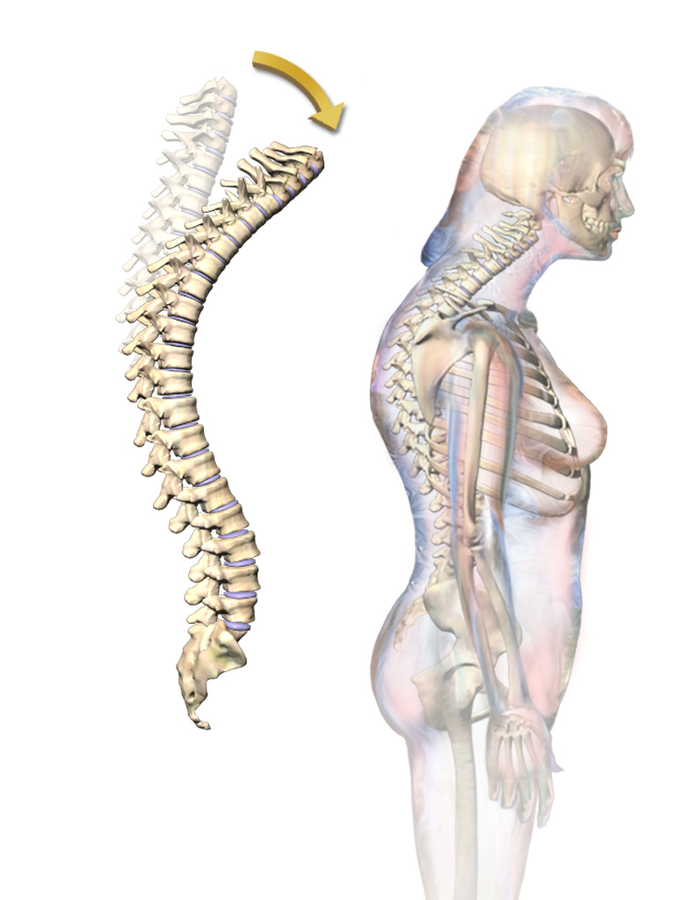
Additionally, when viewing the spine from the side, the thoracic region shows a forward curvature known as kyphosis, while the lumbar region has a backward curvature called lordosis. This morphology is normal for the spine and allows it to better support the body's weight.
When there is scoliosis or when thoracic kyphosis is above normal (meaning the curvature is more pronounced), musculoskeletal pain in that area, respiratory issues (due to lung compression), and even digestive problems (such as difficulty swallowing due to esophageal compression) may arise.
To maintain an appropriate spinal alignment, it is important for the patient to walk or at least spend a minimal amount of time standing each day. This is because when we walk or stand, gravity encourages the body to naturally maintain a centered axis for balance. If the spine were tilted or excessively bent forward or backward while standing or walking, we would continuously fall and struggle to maintain balance. However, sitting makes it easier to keep balance, which may lead to leaning the spine and developing scoliosis.
Similar to other neurological conditions in children, kyphoscoliosis in Kabuki Syndrome can be secondary to joint hyperlaxity and/or potential vertebral defects, along with psychomotor delay and hypotonia. With low muscle tone, the muscles exert little resting force on the bones, which promotes poor skeletal alignment.
In medical literature, kyphosis is documented in about 50% of individuals with SK of various ages and can be either postural or structural.
As for scoliosis, a prevalence of 35% is estimated, observed when there is a lateral curve greater than 10º accompanied by vertebral rotation. It is advisable to conduct imaging tests such as spinal X-rays, and in some cases MRI, to rule out associated vertebral anomalies like hemivertebrae or "butterfly" vertebrae.
Treatment
The best treatment for kyphoscoliosis is prevention through physiotherapy and rehabilitation, especially by promoting postural education, specific physiotherapy treatment, and, though less common, the use of orthopedic devices that aid walking (such as walkers) and standing (like standing frames and inclined planes). It is also crucial to continue these exercises at home for good outcomes. If these measures are insufficient, the use of braces may be considered, or in cases of significant deformity, corrective surgery may be attempted (using titanium rods to fuse the spine, compensating for the curvature and preventing progressive worsening of the deformity).
2.2.2. Hips subluxation
Hip dislocation is the complete loss of contact between the femoral head and the acetabulum (the part of the pelvis where it fits). When the loss of contact is not total but partial, it is referred to as subluxation.
Hip subluxation is relatively common in children with voluntary motor system injuries at the cerebral level (first motor neuron of the pyramidal pathway). The condition most frequently associated with this is cerebral palsy. These children exhibit a type of hypertonia called spasticity, which causes them to maintain very rigid leg postures, making it easier for the femoral head to move out of its normal position.

In individuals with Kabuki Syndrome (SK), there is no hypertonia but hypotonia; thus, hip subluxation should not be a common complication. However, it may occur in children who require prolonged use of a wheelchair.
Symptoms of hip subluxation typically include:
-
Pain during movement (when transferring the patient from sitting to lying down and vice versa, or during daily hygiene)
-
Differences in position between the hips
-
Slight shortening of the affected leg
-
Difficulty sitting comfortably
-
Limping or complete refusal to walk (if they are able to walk)
In some cases, pain may be more challenging to identify as it can be located in the lower back, knee, or calf.
Prevention focuses on ensuring proper posture while sitting (using adjustable seats) or lying down. If the subluxation is significant and painful, hip surgery may be an appropriate option. The most commonly used technique is varus osteotomy of the femoral head with acetabular reconstruction, which has shown good results when performed by a specialized surgeon.
2.2.3. Femoral anteversion
Femoral anteversion is a condition where the femoral neck tilts forward, causing the lower leg to turn inward. It usually corrects itself over time. Therefore, femoral anteversion that results in an inward foot position during walking in children typically does not require any treatment. It resolves spontaneously as they grow. The focus should be on providing recommendations to ensure that this developmental phase remains just that—a normal stage in their growth.
Recommendations for Prevention
-
Infants should not be placed on their stomachs in the crib to avoid forcing hip anteversion.
-
Once children are a bit older and start sitting (especially on the floor), it's crucial they avoid sitting in an "W" position (with legs outward, see figure). This position prevents the gradual reduction of femoral anteversion as they grow.
-

-
Instead, they should sit cross-legged (like sitting "Indian-style", figure 8) and avoid tucking their feet under their buttocks when seated in chairs or sitting on their heels when kneeling.
-
No orthopedic treatments have been found to correct femoral anteversion. Patience is essential as normal development will gradually correct femoral torsion. It's important to emphasize proper sitting posture to support this natural trend toward correction.
2.2.4. Genu valgum
Genu valgum is the lateral deviation of the legs, such that when the knees are brought together, the feet remain apart (also known as "knock-knees" or "X-legs"). This arching is normal between the ages of 3 and 4, in some older girls, and in obese individuals. It is considered pathological when the angle of the knees exceeds specific values for age.

Los niños con síndrome de Kabuki, debido a su hipotonía e hiperlaxitud, pueden presentar genu valgo, que en algunos casos puede ser susceptible de corrección ortopédica. Las plantillas, férulas u otros dispositivos no son necesarios ni efectivos en la mayoría de ocasiones. En aquellos casos en que el genu varo o piernas arqueadas no mejore a los 2-3 años, o siga el genu valgo con más de 9 años, deberán ser derivados a un traumatólogo infantil.
2.2.5. Flat feet
Flat feet are defined as feet that have a significant absence or reduction of the arch. There are two types: flexible flat feet and rigid flat feet. Flexible flat feet are commonly present in most infants, many children under 6 years old, and in 10% of adults. In young children, this is due to the greater amount of plantar fat, increased flexibility of the joints, and lower muscle tone and strength. This type of flat foot tends to correct itself with age and usually does not require treatment.

However, many children with neurological conditions are hypotonic and therefore may have flexible flat feet. In children with Kabuki syndrome, due to hyperlaxity and this hypotonia, there is often flexible flat foot. While treatment is usually not necessary in the general population, in children with Kabuki syndrome, insoles or ankle-foot orthoses (AFOs) can be helpful when they have difficulty walking. These devices promote better ankle alignment and facilitate walking.